
Abstract
Risks associated with fatigue that accumulates during work shifts have historically been managed through working time arrangements that specify fixed maximum durations of work shifts and minimum durations of time off. By themselves, such arrangements are not sufficient to curb risks to performance, safety, and health caused by misalignment between work schedules and the biological regulation of waking alertness and sleep. Science-based approaches for determining shift duration and mitigating associated risks, while addressing operational needs, require: (1) a recognition of the factors contributing to fatigue and fatigue-related risks; (2) an understanding of evidence-based countermeasures that may reduce fatigue and/or fatigue-related risks; and (3) an informed approach to selecting workplace-specific strategies for managing work hours. We propose a series of guiding principles to assist stakeholders with designing a shift duration decision-making process that effectively balances the need to meet operational demands with the need to manage fatigue-related risks.

Similar content being viewed by others

REFERENCES
Skeiky L, et al. Circadian rhythms in sleepiness, alertness, and performance. In: Kryger MH, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 7th ed. Philadelphia: Elsevier, in press.
Pigeon WR, et al. Distinguishing between excessive daytime sleepiness and fatigue: toward improved discovery and treatment. J Psychosom Res. 2003;54(1):61–69.
Shen J, et al. Distinguishing sleepiness and fatigue: focus on definition and measurement. Sleep Med Rev. 2006;10(1):63–76.
Åkerstedt T. Consensus statement: fatigue and accidents in transport operations. J Sleep Res. 2000;9(4):395.
Satterfield BC, et al. Occupational fatigue, underlying sleep and circadian mechanisms, and approaches to fatigue risk management. Fatigue Biomed Health Behav 2013;1:118–136.
IATA, ICAO, IFALPA. Fatigue Risk Management Systems Implementation Guide for Operators. 1st ed. 2011. https://www.icao.int/safety/fatiguemanagement/FRMS%20Tools/FRMS%20Implementation%20Guide%20for%20Operators%20July%202011.pdf (last accessed on March 30, 2021).
Van Dongen HPA, et al. Alertness level. In: Binder MD, Hirokawa N, Windhorst U, eds. Encyclopedia of Neuroscience. Berlin: Springer, 2008:75–77.
Wong IS, et al. International consensus statements on non-standard working time arrangements and occupational health and safety. Ind Health. 2019;57(2):135–138.
Arlinghaus A, et al. Working time society consensus statements: evidence-based effects of shift work and non-standard working hours on workers, family and community. Ind Health. 2019;57(2):184–200.
Moreno CRC, et al. Working time society consensus statements: evidence-based effects of shift work on physical and mental health. Ind Health. 2019;57(2):139–157.
Honn KA, et al. Working time society consensus statements: prescriptive rule sets and risk management-based approaches for the management of fatigue-related risk in working time arrangements. Ind Health. 2019;57(2):264–280.
Mackworth NH. Researches on the Measurement of Human Performance. Medical Research Council Special Report Series. London: Privy Council, 1950.
Åkerstedt T. Work hours, sleepiness and the underlying mechanisms. J Sleep Res. 1995;4(S2):15–22.
Johnson JV, et al. Long working hours, occupational health and the changing nature of work organization. Am J Ind Med. 2006;49(11):921–929.
Burke RJ, et al. The Long Work Hours Culture: Causes, Consequences and Choices. 1st ed. Bingley: Emerald Group Publishing; 2008.
US Bureau of Labor Statistics. Job flexibilities and work schedules summary. 2019, https://www.bls.gov/news.release/flex2.nr0.htm (last accessed on March 30, 2021).
US Bureau of Labor Statistics. Labor force statistics from the Current Population Survey. 2020, https://www.bls.gov/cps/lfcharacteristics.htm#hours (last accessed on March 30, 2021).
Belzer MH. The economics of long work hours: how economic incentives influence workplace practice. Ind Health. 2020;58(5):399–402.
McMenamin T. A time to work: recent trends in shift work and flexible schedules. Monthly Labor Rev. 2007;130(12):3–15.
Shockey TM, et al. Short sleep duration by occupation group– 29 states, 2013–2014. Morbid Mortal Weekly Rep. 2017;66(8):207–213.
Basner M, et al. Sociodemographic characteristics and waking activities and their role in the timing and duration of sleep. Sleep. 2014;37(12):1889–1906.
Marucci-Wellman HR, et al. Differences in time use and activity patterns when adding a second job: implications for health and safety in the United States. Am J Public Health. 2014;104(8):1488–1500.
Wong IS, et al. Working Time Society consensus statements: a multi-level approach to managing occupational sleep- related fatigue. Ind Health. 2019;57(2):228–244.
Riedy S, et al. Fatigue and short-term unplanned absences among police officers. Policing. 2020;43(3):483–494.
Harrison Y, et al. The impact of sleep deprivation on decision making: a review. J Exp Psychol Appl. 2000;6(3):236–249.
Ricci JA, et al. Fatigue in the U.S. workforce: prevalence and implications for lost productive work time. J Occup Environ Med. 2007;49(1):1–10.
Landrigan CP, et al. Effect of reducing interns’ work hours on serious medical errors in intensive care units. N Engl J Med. 2004;351(18):1838–1848.
Fischer FM, et al. Working Time Society consensus statements: psychosocial stressors relevant to the health and wellbeing of night and shift workers. Ind Health. 2019;57(2):175–183.
Banks S, et al. Effects of fatigue on teams and their role in 24/7 operations. Sleep Med Rev. 2019;48:101216.
Killgore WDS. Effects of sleep deprivation on cognition. Prog Brain Res. 2010;185:105–129.
Barnes CM, et al. Lack of sleep and unethical behavior. Organ Behav Hum Decis Proc. 2011;115:169–180.
Estryn-Béhar M, et al.; NEXT Study Group. Effects of extended work shifts on employee fatigue, health, satisfaction, work/family balance, and patient safety. Work. 2012;41(Suppl 1):4283–4290.
Bell LB, et al. Effects of 13-hour 20-minute work shifts on law enforcement officers’ sleep, cognitive abilities, health, quality of life, and work performance: the Phoenix Study. Police Q. 2015;18(3):293–337.
Bazazan A, et al. Fatigue as a mediator of the relationship between quality of life and mental health problems in hospital nurses. Accid Anal Prev. 2019;126:31–36.
Williamson A, et al. The link between fatigue and safety. Accid Anal Prev. 2011;43(2):498–515.
Good CH, et al. Sleep in the United States Military. Neuropsychopharmacology. 2020;45(1):176–191.
Dembe AE, et al. The impact of overtime and long work hours on occupational injuries and illnesses: new evidence from the United States. Occup Environ Med. 2005;62(9):588–597.
Wagstaff AS, et al. Shift and night work and long working hours—a systematic review of safety implications. Scand J Work Environ Health. 2011;37(3):173–185.
Dawson D, et al. How much sleep do you need? A comprehensive review of fatigue related impairment and the capacity to work or drive safely. Accid Anal Prev. 2021;151:105955.
Barger LK, et al.; Harvard Work Hours, Health, and Safety Group. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352(2):125–134.
Mitler MM, et al. Catastrophes, sleep, and public policy: consensus report. Sleep. 1988;11(1):100–109.
Dinges DF. An overview of sleepiness and accidents. J Sleep Res. 1995;4(S2): 4–14.
Rivera AS, et al. Shift work and long work hours and their association with chronic health conditions: a systematic review of systematic reviews with meta-analyses. PLoS One. 2020;15(4):e0231037.
Caruso CC, et al. Long working hours, safety, and health: toward a National Research Agenda. Am J Ind Med. 2006;49(11):930–942.
Rosekind MR. Underestimating the societal costs of impaired alertness: safety, health and productivity risks. Sleep Med. 2005;6(Suppl 1):S21–S25.
Price JM, et al. A method for applying fatigue science to accident investigation. Rev Hum Factors Ergon. 2015;10: 79–114.
Dawson D, et al. Determining the likelihood that fatigue was present in a road accident: a theoretical review and suggested accident taxonomy. Sleep Med Rev. 2018;42:202–210.
Dijk DJ, et al. Circadian and sleep/wake dependent aspects of subjective alertness and cognitive performance. J Sleep Res. 1992;1(2):112–117.
Gander PH. Evolving regulatory approaches for managing fatigue risk in transportation operations. Rev Hum Factors Ergon. 2015;10: 253–271.
Flynn-Evans EE, et al.; American Academy of Sleep Medicine Public Safety Committee. Industrial regulation of fatigue: lessons learned from aviation. J Clin Sleep Med. 2019;15(4):537–538.
Patterson PD, et al. Shorter versus longer shift durations to mitigate fatigue and fatigue-related risks in emergency medical services personnel and related shift workers: a systematic review. Prehosp Emerg Care. 2018;22(Suppl 1):28–36.
Patterson PD, et al. Evidence-based guidelines for fatigue risk management in emergency medical services. Prehosp Emerg Care. 2018;22(Suppl 1):89–101.
Lee S, et al. Working Time Around the World: Trends in Working Hours, Laws and Policies in a Global Comparative Perspective.. Geneva: International Labour Office; 2007.
Gärtner J, et al. Working Time Society consensus statements: regulatory approaches to reduce risks associated with shift work-a global comparison. Ind Health. 2019;57(2):245–263.
Kecklund G, et al. Health consequences of shift work and insufficient sleep. BMJ. 2016;355:i5210.
Grandou C, et al. The effects of sleep loss on military physical performance. Sports Med. 2019;49(8):1159–1172.
Jackson ML, et al. Deconstructing and reconstructing cognitive performance in sleep deprivation. Sleep Med Rev. 2013;17(3):215–225.
Barnes CM, et al. Too tired to inspire or be inspired: sleep deprivation and charismatic leadership. J Appl Psychol. 2016;101(8):1191–1199.
Maia Q, et al. Short and long sleep duration and risk of drowsy driving and the role of subjective sleep insufficiency. Accid Anal Prev. 2013;59:618–622.
Caldwell JA, et al. Fatigue and its management in the workplace. Neurosci Biobehav Rev. 2019;96:272–289.
Borbély AA, et al. Sleep homeostasis and models of sleep regulation. J Biol Rhythms.. 1999;14(6):557–568.
Van Dongen HPA, et al. Sleep, circadian rhythms, and psychomotor vigilance. Clin Sports Med. 2005;24(2):237–49, vii.
Basner M, et al. American time use survey: sleep time and its relationship to waking activities. Sleep. 2007;30(9):1085–1095.
Shattuck NL, et al. Does the quality of life differ for shift workers compared to day workers? Chronobiol Int. 2020;37(9–10):1299–1303.
Belenky G, et al. Patterns of performance degradation and restoration during sleep restriction and subsequent recovery: a sleep dose-response study. J Sleep Res. 2003;12(1):1–12.
Van Dongen HPA, et al. The cumulative cost of additional wakefulness: dose-response effects on neurobehavioral functions and sleep physiology from chronic sleep restriction and total sleep deprivation. Sleep. 2003;26(2):117–126.
Grech MR, et al. An examination of the relationship between workload and fatigue within and across consecutive days of work: is the relationship static or dynamic? J Occup Health Psychol. 2009;14(3):231–242.
Åkerstedt T, et al. Do sleep, stress, and illness explain daily variations in fatigue? A prospective study. J Psychosom Res. 2014;76(4):280–285.
Sparrow AR, et al. Drowsiness measures for commercial motor vehicle operations. Accid Anal Prev. 2019;126:146–159.
Dawson D, et al. Safety implications of fatigue and sleep inertia for emergency services personnel. Sleep Med Rev. 2021;55:101386.
Baron KG, et al. Circadian misalignment and health. Int Rev Psychiatry. 2014;26(2):139–154.
Boivin DB, et al. Impacts of shift work on sleep and circadian rhythms. Pathol Biol (Paris). 2014;62(5):292–301.
James SM, et al. Shift work: disrupted circadian rhythms and sleep-implications for health and well-being. Curr Sleep Med Rep. 2017;3(2):104–112.
Soccolich SA, et al. An analysis of driving and working hour on commercial motor vehicle driver safety using naturalistic data collection. Accid Anal Prev. 2013;58:249–258.
Van Dongen HPA, et al. The efficacy of a restart break for recycling with optimal performance depends critically on circadian timing. Sleep. 2011;34(7):917–929.
Sparrow AR, et al. Naturalistic field study of the restart break in US commercial motor vehicle drivers: truck driving, sleep, and fatigue. Accid Anal Prev. 2016;93:55–64.
Flynn-Evans EE, et al. Sleep and neurobehavioral performance vary by work start time during non-traditional day shifts. SleepHealth. 2018;4(5):476–484.
Muecke S. Effects of rotating night shifts: literature review. J Adv Nurs. 2005;50(4):433–439.
Sallinen M, et al. Shift work, sleep, and sleepiness - differences between shift schedules and systems. Scand J Work Environ Health. 2010;36(2):121–133.
Dall’Ora C, et al. Characteristics of shift work and their impact on employee performance and wellbeing: a literature review. Int J Nurs Stud. 2016;57:12–27.
Williamson A, Friswell R. Fatigue in the workplace: causes and countermeasures. FatigueBiomed Health Behav. 2013;1:81–98.
Folkard S, et al. Shift work, safety and productivity. Occup Med (Lond). 2003;53(2):95–101.
Kandelaars KJ, et al. The impact of extended leave on sleep and alertness in the Australian rail industry. IndHealth. 2005;43(1):105–113.
van den Berg TI, et al. The effects of work-related and individual factors on the Work Ability Index: a systematic review. Occup Environ Med. 2009;66(4):211–220.
Henderson A. Emotional labor and nursing: an under-appreciated aspect of caring work. Nurs Inq. 2001;8(2):130–138.
Honn KA, et al. Fatiguing effect of multiple take-offs and landings in regional airline operations. Accid Anal Prev. 2016;86:199–208.
Arsintescu L, et al. The relationship between workload, performance and fatigue in a short-haul airline. Chronobiol Int. 2020;37(9–10):1492–1494.
Jackson JE, et al. Fatigue in highway construction workers: Risks and countermeasures in rapid renewal project schedules. Transp Res Rec. 2013;2347:11–18.
Dekker S. Just Culture: Balancing Safety and Accountability. 2nd ed. Burlington: Ashgate Publishing, 2008.
Briner RB. Relationships between work environments, psychological environments and psychological well-being. Occup Med (Lond). 2000;50(5):299–303.
Dawson D, et al. Fatigue-proofing: a new approach to reducing fatigue-related risk using the principles of error management. Sleep Med Rev. 2012;16(2):167–175.
Higgins JS, et al. Asleep at the wheel - the road to addressing drowsy driving. Sleep. 2017;40:zsx001.
Matsangas P, et al. Sleep quality, occupational factors, and psychomotor vigilance performance in U.S. Navy sailors. Sleep. 2020;43:zsaa118.
Petrov ME, et al. Commuting and sleep: results from the Hispanic community health study/study of Latinos Sueño ancillary study. Am J Prev Med. 2018;54(3):e49–e57.
Ritonja J, et al. Working Time Society consensus statements: individual differences in shift work tolerance and recommendations for research and practice. IndHealth. 2019;57(2):201–212.
Kerkhof GA. Inter-individual differences in the human circadian system: a review. Biol Psychol. 1985;20(2):83–112.
Vetter C, et al. Aligning work and circadian time in shift workers improves sleep and reduces circadian disruption. Curr Biol. 2015;25(7):907–911.
Härmä M. Individual differences in tolerance to shiftwork: a review. Ergonomics. 1993;36(1–3):101–109.
Härmä M. Ageing, physical fitness and shiftwork tolerance. Appl Ergon. 1996;27(1):25–29.
Wirtz A, et al. Gender differences in the effect of weekly working hours on occupational injury risk in the United States working population. Scand J Work Environ Health. 2012;38(4):349–357.
Baillargeon J. Characteristics of the healthy worker effect. Occup Med. 2001;16(2):359–366.
Van Dongen HPA. Shift work and inter-individual differences in sleep and sleepiness. Chronobiol Int. 2006;23(6):1139–1147.
Kalmbach DA, et al. The impact of stress on sleep: pathogenic sleep reactivity as a vulnerability to insomnia and circadian disorders. J Sleep Res. 2018;27(6):e12710.
Tucker P, et al. Review of studies that have used the Standard Shiftwork Index: evidence for the underlying model of shiftwork and health. Appl Ergon. 2008;39(5):550–564.
Watson NF, et al. Joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society on the recommended amount of sleep for a healthy adult: Methodology and discussion. Sleep. 2015;38(6):1161–1183.
Watson NF, et al. Recommended amount of sleep for a healthy adult: a joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep. 2015;38(6):843–844.
Rosekind MR, et al. Managing fatigue in operational settings. 1: physiological considerations and countermeasures. Behav Med. 1996;21(4):157–165.
Redeker NS, et al. Workplace interventions to promote sleep health and an alert, healthy workforce. J Clin Sleep Med. 2019;15(4):649–657.
Rangan S, et al. Predictive and proactive fatigue risk management approaches in commercial aviation. Chronobiol Int. 2020;37(9–10):1479–1482.
Roehrs T, et al. Caffeine: sleep and daytime sleepiness. Sleep Med Rev. 2008;12(2):153–162.
Temple JL, et al. Systematic review and meta-analysis of the effects of caffeine in fatigued shift workers: implications for emergency medical services personnel. Prehosp Emerg Care. 2018;22(sup1):37–46.
Drake C, et al. Caffeine effects on sleep taken 0, 3, or 6 hours before going to bed. J Clin Sleep Med. 2013;9(11):1195–1200.
Martin-Gill C, et al. Effects of napping during shift work on sleepiness and performance in emergency medical services personnel and similar shift workers: a systematic review and meta-analysis. Prehosp Emerg Care. 2018;22(sup1):47–57.
Alger SE, et al. Challenging the stigma of workplace napping. Sleep. 2019;42:zsz097.
Hilditch CJ, et al. Sleep inertia: current insights. Nat Sci Sleep. 2019;11:155–165.
Snel J, et al. Effects of caffeine on sleep and cognition. Prog Brain Res. 2011;190:105–117.
Milner CE, et al. Benefits of napping in healthy adults: impact of nap length, time of day, age, and experience with napping. J Sleep Res. 2009;18(2):272–281.
Vital-Lopez FG, et al. Caffeine dosing strategies to optimize alertness during sleep loss. J Sleep Res. 2018;27(5):e12711.
Lovato N, et al. The effects of napping on cognitive functioning. Prog Brain Res. 2010;185:155–166.
Commissaris DACM, et al. Interventions to reduce sedentary behavior and increase physical activity during productive work: a systematic review. Scand J Work Environ Health. 2016;42(3):181–191.
Gander P, et al. Fatigue risk management: organizational factors at the regulatory and industry/company level. Accid Anal Prev. 2011;43(2):573–590.
Barger LK, et al. Effect of fatigue training on safety, fatigue, and sleep in emergency medical services personnel and other shift workers: a systematic review and meta-analysis. Prehosp Emerg Care. 2018;22(Suppl 1):58–68.
Davenport N, Lowry C, Pinkston B. Use of stimulants in operational settings: Issues and considerations. In Wesensten NJ ed., Sleep Deprivation, Stimulant Medications, and Cognition. Cambridge University Press, Cambridge; 2012: 237–256.
Lerman SE, et al.; American College of Occupational and Environmental Medicine Presidential Task Force on Fatigue Risk Management. Fatigue risk management in the workplace. J Occup Environ Med. 2012;54(2):231–258.
Coplen MK, et al. From transportation fatigue research to effective practice: the case for evaluation. Rev Hum Fact Ergon. 2015;10:272–302.
Dawson D, et al. Managing fatigue: it’s about sleep. Sleep Med Rev. 2005;9(5):365–380.
Wilson M, et al. Sleep quality, sleepiness and the influence of workplace breaks: a cross-sectional survey of health-care workers in two US hospitals. Chronobiol Int. 2018;35(6):849–852.
Balkin TJ, et al. The process of awakening: a PET study of regional brain activity patterns mediating the re-establishment of alertness and consciousness. Brain. 2002;125(Pt 10):2308–2319.
Hilditch CJ, et al. Time to wake up: reactive countermeasures to sleep inertia. Ind Health. 2016;54(6):528–541.
International Organization for Standardization. Risk Management - Guidelines. 2nd ed. (ISO Standard No. 31000:2018). Geneva: ISO Copyright Office; 2018.
Borbély AA. A two process model of sleep regulation. Hum Neurobiol. 1982;1(3):195–204.
Daan S, et al. Timing of human sleep: recovery process gated by a circadian pacemaker. Am J Physiol. 1984;246(2 Pt 2):R161–R183.
Dijk DJ, et al. Paradoxical timing of the circadian rhythm of sleep propensity serves to consolidate sleep and wakefulness in humans. Neurosci Lett. 1994;166(1): 63–68.
Lavie P. Ultrashort sleep-waking schedule. III. 'Gates’ and 'forbidden zones’ for sleep. Electroencephalogr Clin Neurophysiol. 1986;63(5):414–425.
Strogatz SH, et al. Circadian pacemaker interferes with sleep onset at specific times each day: role in insomnia. Am J Physiol. 1987;253(1 Pt 2):R172–R178.
Barger LK, et al. Neurobehavioral, health, and safety consequences associated with shift work in safety-sensitive professions. Curr Neurol Neurosci Rep. 2009;9(2):155–164.
Fischer D, et al. Updating the “Risk Index”: a systematic review and meta-analysis of occupational injuries and work schedule characteristics. Chronobiol Int. 2017;34(10):1423–1438.
Knutsson A. Methodological aspects of shift-work research. Chronobiol Int. 2004;21(6):1037–1047.
Driscoll TR, et al. A systematic review of the neurobehavioural and physiological effects of shiftwork systems. Sleep Med Rev. 2007;11(3):179–194.
Lockley SW, et al.; Harvard Work Hours, Health and Safety Group. Effects of health care provider work hours and sleep deprivation on safety and performance. Jt Comm J Qual Patient Saf. 2007;33(11 Suppl):7–18.
Smith L, et al. Work shift duration: a review comparing eight hour and 12 hour shift systems. Occup Environ Med. 1998;55(4):217–229.
Folkard S, et al. Trends in the risk of accidents and injuries and their implications for models of fatigue and performance. Aviat Space Environ Med. 2004;75(3 Suppl):A161–A167.
Geiger-Brown J, et al. Sleep, sleepiness, fatigue, and performance of 12-hour-shift nurses. Chronobiol Int. 2012;29(2):211–219.
Vila B, Samuels C. Sleep loss in first responders and the military. In: Kryger MH, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 5th ed. St. Louis: Elsevier Saunders, 2011:799–808.
Min A, et al. Work schedule characteristics and fatigue among rotating shift nurses in hospital setting: an integrative review. J Nurs Manag. 2019;27(5):884–895.
Ferguson SA, et al. On-call work: to sleep or not to sleep? it depends. Chronobiol Int. 2016;33(6):678–684.
Alghamdi MG. Nursing workload: a concept analysis. J Nurs Manag. 2016;24(4):449–457.
Studnek JR, et al. Effect of task load interventions on fatigue in emergency medical services personnel and other shift workers: a systematic review. Prehosp Emerg Care. 2018;22(sup1):81–88.
Dinges DF, et al. The benefits of a nap during prolonged work and wakefulness. Work Stress. 1998;2:139–153.
Mollicone DJ, et al. Response surface mapping of neurobehavioral performance: testing the feasibility of split sleep schedules for space operations. Acta Astronaut. 2008;63(7–10):833–840.
Ficca G, et al. Naps, cognition and performance. Sleep Med Rev. 2010;14(4): 249–258.
Faraut B, et al. Napping: a public health issue. From epidemiological to laboratory studies. Sleep Med Rev. 2017;35:85–100.
Ruggiero JS, et al. Effects of napping on sleepiness and sleep-related performance deficits in night-shift workers: a systematic review. Biol Res Nurs. 2014;16(2):134–142.
Dinges DF, et al. Temporal placement of a nap for alertness: contributions of circadian phase and prior wakefulness. Sleep. 1987;10(4):313–329.
Gillberg M, et al. The effects of a short daytime nap after restricted night sleep. Sleep. 1996;19(7):570–575.
Sallinen M, et al. Promoting alertness with a short nap during a night shift. ] Sleep Res. 1998;7(4):240–247.
Matsumoto K, et al. The effect of night-time naps on recovery from fatigue following night work. Ergonomics. 1994;37(5):899–907.
Garbarino S, et al. Professional shift-work drivers who adopt prophylactic naps can reduce the risk of car accidents during night work. Sleep. 2004;27(7):1295–1302.
Rotenberg L, et al. Work schedule and self-reported hypertension - the potential beneficial role of on-shift naps for night workers. Chronobiol Int. 2016;33(6):697–705.
Patterson PD, et al. Ambulatory blood pressure monitoring among emergency medical services night shift workers. Occup Environ Med. 2021;78(1):29–35.
Zhou X, et al. Do split sleep/wake schedules reduce or increase sleepiness for continuous operations? Accid Anal Prev. 2017;99(Pt B):434–439.
Kosmadopoulos A, et al. The effects of a split sleep-wake schedule on neurobehavioural performance and predictions of performance under conditions of forced desynchrony. Chronobiol Int. 2014;31(10):1209–1217.
Short MA, et al. The effect of split sleep schedules (6 h-on/6 h-off) on neurobehavioural performance, sleep and sleepiness. Appl Ergon. 2016;54:72–82.
Geiger-Brown J, et al. CE: original research: napping on the night shift: a two-hospital implementation project. Am J Nurs. 2016;116(5):26–33.
Tassi P, et al. Sleep inertia. SleepMed Rev. 2000;4(4):341–353.
Dinges DF, et al. Performance after naps in sleep-conducive and alerting environments. In: Johnson LC, ed. Biological Rhythms, Sleep and Shift Work: Advances in Sleep Research Vol. 7. New York: Spectrum; 1981:539–552.
Ferrara M, et al. Time-course of sleep inertia upon awakening from nighttime sleep with different sleep homeostasis conditions. Aviat Space Environ Med. 2000;71(3):225–229.
Hilditch CJ, et al. A review of short naps and sleep inertia: do naps of 30 min or less really avoid sleep inertia and slow- wave sleep? Sleep Med. 2017;32:176–190.
Bonnet MH, et al. Utility of caffeine: Evidence from the laboratory. In: Wesensten NJ, ed. Sleep Deprivation, Stimulant Medications, and Cognition. New York: Cambridge University Press, 2012:82–92.
Reyner LA, et al. Suppression of sleepiness in drivers: combination of caffeine with a short nap. Psychophysiology. 1997;34(6):721–725.
Van Dongen HPA, et al. Caffeine eliminates psychomotor vigilance deficits from sleep inertia. Sleep. 2001;24(7):813–819.
Newman RA, et al. Caffeine gum minimizes sleep inertia. Percept Mot Skills. 2013;116(1):280–293.
Centofanti S, et al. A pilot study investigating the impact of a caffeine-nap on alertness during a simulated night shift. Chronobiol Int. 2020;37(9–10): 1469–1473.
van Dam RM, et al. Coffee, caffeine, and health. N Engl J Med. 2020;383(4): 369–378.
Evans SM, et al. Caffeine tolerance and choice in humans. Psychopharmacology (Berl). 1992;108(1–2):51–59.
Quartana PJ, et al. Genetic basis of individual vulnerability to sleep loss and responsivity to stimulants. In: Wesensten NJ, ed. Sleep Deprivation, Stimulant Medications, and Cognition. New York: Cambridge University Press; 2012:43–57.
Spaeth AM, et al. Cumulative neurobehavioral and physiological effects of chronic caffeine intake: individual differences and implications for the use of caffeinated energy products. Nutr Rev. 2014;72(Suppl 1):34–47.
Clark I, et al. Coffee, caffeine, and sleep: a systematic review of epidemiological studies and randomized controlled trials. Sleep Med Rev.. 2017;31:70–78.
Leonard TK, et al. The effects of caffeine on various body systems: a review. J Am Diet Assoc. 1987;87(8):1048–1053.
Bruce M, et al. Caffeine withdrawal: a contrast of withdrawal symptoms in normal subjects who have abstained from caffeine for 24 hours and for 7 days. J Psychopharmacol. 1991;5(2):129–134.
Wikoff D, et al. Systematic review of the potential adverse effects of caffeine consumption in healthy adults, pregnant women, adolescents, and children. Food Chem Toxicol. 2017;109(Pt 1):585–648.
Shahly V, et al. The associations of insomnia with costly workplace accidents and errors: results from the America Insomnia Survey. Arch Gen Psychiatry. 2012;69(10):1054–1063.
Hauri P. Sleep hygiene. In: Hauri P, ed. Current Concepts: The Sleep Disorders. Kalamazoo, MI: Upjohn Company, 1977:21–35.
Rupp TL, et al. Banking sleep: realization of benefits during subsequent sleep restriction and recovery. Sleep. 2009;32(3):311–321.
Patterson PD, et al. Does evidence support “banking/ex- tending sleep” by shift workers to mitigate fatigue, and/or to improve health, safety, or performance? A systematic review. Sleep Health. 2019;5(4):359–369.
Caddick ZA, et al. A review of the environmental parameters necessary for an optimal sleep environment. Build Environ. 2018;132:11–20.
Stepanski EJ, et al. Use of sleep hygiene in the treatment of insomnia. Sleep Med Rev. 2003;7(3):215–225.
Irish LA, et al. The role of sleep hygiene in promoting public health: a review of empirical evidence. Sleep Med Rev. 2015;22:23–36.
Bixler EO, et al. Excessive daytime sleepiness in a general population sample: the role of sleep apnea, age, obesity, diabetes, and depression. J Clin Endocrinol Metab. 2005;90(8):4510–4515.
Pagel JF. Drug-induced hypersomnolence. Sleep Med Clin. 2017;12(3):383–393.
Melamed S, et al. Excessive daytime sleepiness and risk of occupational injuries in non-shift daytime workers. Sleep. 2002;25(3):315–322.
Burks SV, et al. Nonadherence with employer-mandated sleep apnea treatment and increased risk of serious truck crashes. Sleep. 2016;39(5):967–975.
Burks SV, et al. Employer-mandated obstructive sleep apnea treatment and healthcare cost savings among truckers. Sleep. 2020;43:zsz262.
Czeisler CA, et al.; U. S. Modafinil in Shift Work Sleep Disorder Study Group. Modafinil for excessive sleepiness associated with shift-work sleep disorder. N Engl J Med. 2005;353(5):476–486.
Sateia MJ, et al. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: an American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13(2):307–349.
Caldwell JA. Optimizing alertness with medications: The case for hypnotics. In: Ackerman PL, ed. Cognitive Fatigue: Multidisciplinary Perspectives on Current Research and Future Applications. Washington, D.C.: American Psychological Association; 2011:231–246.
Gill M, et al. Cognitive performance following modafinil versus placebo in sleep-deprived emergency physicians: a double-blind randomized crossover study. Acad Emerg Med. 2006;13(2):158–165.
van der Sluiszen NNJJM, et al. Driving performance and neurocognitive skills of long-term users of benzodiazepine anxiolytics and hypnotics. Hum Psychopharmacol. 2019;34(6):e2715.
Johnson LC, et al. Benzodiazepines and caffeine: effect on daytime sleepiness, performance, and mood. Psychopharmacology (Berl). 1990;101(2):160–167.
Cressman AM, et al.; Canadian Drug Safety and Effectiveness Research Network. Prescription stimulant use and hospitalization for psychosis or mania: a population-based study. J Clin Psychopharmacol. 2015;35(6):667–671.
Roth T, et al. Pharmacological effects of sedative-hypnotics, narcotic analgesics, and alcohol during sleep. Med Clin North Am. 1985;69(6):1281–1288.
Roehrs T, et al. Sleep, sleepiness, and alcohol use. Alcohol Res Health. 2001;25(2):101–109.
Auld F, et al. Evidence for the efficacy of melatonin in the treatment of primary adult sleep disorders. Sleep Med Rev. 2017;34:10–22.
Sharkey KM, et al. Effects of melatonin administration on daytime sleep after simulated night shift work. J Sleep Res. 2001;10(3):181–192.
Herxheimer A, et al. Melatonin for the prevention and treatment of jet lag. Cochrane Database Syst Rev. 2002;2:CD001520.
Lewy AJ, et al. Melatonin shifts human circadian rhythms according to a phase-response curve. Chronobiol Int. 1992;9(5):380–392.
Andersen LP, et al. The safety of melatonin in humans. Clin Drug Investig. 2016;36(3):169–175.
Chellappa SL, et al. Can light make us bright? Effects of light on cognition and sleep. Prog Brain Res. 2011;190:119–133.
Minors DS, et al. A human phase-response curve to light. Neurosci Lett. 1991;133(1):36–40.
Khalsa SBS, et al. A phase response curve to single bright light pulses in human subjects. J Physiol. 2003;549(Pt 3):945–952.
Boivin DB, et al. Dose-response relationships for resetting of human circadian clock by light. Nature. 1996;379(6565):540–542.
Czeisler CA, et al. Sleep and circadian rhythms in humans. Cold Spring Harb Symp Quant Biol. 2007;72:579–597.
Lockley SW, et al. High sensitivity of the human circadian melatonin rhythm to resetting by short wavelength light. J Clin Endocrinol Metab. 2003;88(9): 4502–4505.
Lee C, et al. A compromise phase position for permanent night shift workers: circadian phase after two night shifts with scheduled sleep and light/dark exposure. Chronobiol Int. 2006;23(4):859–875.
Shechter A, et al. Interventions to reduce short-wavelength (“blue”) light exposure at night and their effects on sleep: a systematic review and meta-analysis. Sleep Adv. 2020:1:zpaa002.
Eastman CI, et al. How to use light and dark to produce circadian adaptation to night shift work. Ann Med. 1999;31(2):87–98.
Cajochen C. Alerting effects of light. Sleep Med Rev. 2007;11(6):453–464.
Smolders KCHJ, et al. Investigation of dose-response relationships for effects of white light exposure on correlates of alertness and executive control during regular daytime working hours. J Biol Rhythms. 2018;33(6):649–661.
Rahman SA, et al. Diurnal spectral sensitivity of the acute alerting effects of light. Sleep. 2014;37(2):271–281.
Phipps-Nelson J, et al. Daytime exposure to bright light, as compared to dim light, decreases sleepiness and improves psychomotor vigilance performance. Sleep. 2003;26(6):695–700.
Viola AU, et al. Blue-enriched white light in the workplace improves self-reported alertness, performance and sleep quality. Scand J Work Environ Health. 2008;34(4):297–306.
Kloog I, et al. Global co-distribution of light at night (LAN) and cancers of prostate, colon, and lung in men. Chronobiol Int. 2009;26(1):108–125.
Yang WS, et al. Light exposure at night, sleep duration, melatonin, and breast cancer: a dose-response analysis of observational studies. Eur J Cancer Prev. 2014;23(4):269–276.
International Agency for Research on Cancer. Night Shift Work. IARC Monographs on the Identification of Carcinogenic Hazards to Humans. vol. 124. Lyon, France: IARC, 2020.
Mainster MA. Light and macular degeneration: a biophysical and clinical perspective. Eye (Lond). 1987;1(Pt 2):304–310.
Tosini G, et al. Effects of blue light on the circadian system and eye physiology. Mol Vis. 2016;22:61–72.
Kredlow MA, et al. The effects of physical activity on sleep: a meta-analytic review. J Behav Med. 2015;38(3):427–449.
Kelley GA, et al. Exercise and sleep: a systematic review of previous meta-analyses. J Evid Based Med. 2017;10(1):26–36.
Stutz J, et al. Effects of evening exercise on sleep in healthy participants: a systematic review and meta-analysis. Sports Med. 2019;49(2):269–287.
Youngstedt SD, et al. Human circadian phase-response curves for exercise. J Physiol. 2019;597(8):2253–2268.
Barger LK, et al. Daily exercise facilitates phase delays of circadian melatonin rhythm in very dim light. Am J Physiol Regul Integr Comp Physiol. 2004;286(6):R1077–R1084.
Matsumoto Y, et al. Physical activity increases the dissociation between subjective sleepiness and objective performance levels during extended wakefulness in human. Neurosci Lett. 2002;326(2):133–136.
Ojo SO, et al. The impact of active workstations on workplace productivity and performance: a systematic review. Int J Environ Res Public Health. 2018;15:417.
Riedy SM, et al. Sleep, sleepiness, and performance prediction modeling. In: Kryger MH, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 7th ed. Philadelphia: Elsevier, in press.
Bianchi MT. Sleep devices: wearables and nearables, informational and interventional, consumer and clinical. Metabolism. 2018;84:99–108.
Abe T, et al. Sleepiness and safety: where biology needs technology. SleepBiol Rhythms.. 2014;12(2):74–84.
Burns M, et al. Fitness-for-duty testing: a new approach to workplace safety. Alcohol Health Res World. 1995;19(2):159–160.
Mallis MM, et al. Summary of the key features of seven biomathematical models of human fatigue and performance. Aviat Space Environ Med. 2004;75(3 Suppl):A4–14.
Van Dongen HPA. Comparison of mathematical model predictions to experimental data of fatigue and performance. Aviat Space Environ Med. 2004;75(3 Suppl):A15–A36.
Rangan S, et al. Integrated fatigue modeling in crew rostering and operations. Can Aeronaut Space J. 2013;59:1–6.
Gunzelmann G, et al. Basic and applied science interactions in fatigue understanding and risk mitigation. Prog Brain Res. 2019;246:177–204.
James FO, et al. Does implementation of biomathematical models mitigate fatigue and fatigue-related risks in emergency medical services operations? a systematic review. Prehosp Emerg Care. 2018;22(sup1):69–80.
Roomkham S, et al. Promises and challenges in the use of consumer-grade devices for sleep monitoring. IEEE Rev Biomed Eng. 2018;11:53–67.
Guillodo E, et al.; HUGOPSY Network. Clinical applications of mobile health wearable-based sleep monitoring: systematic review. JMIR Mhealth Uhealth. 2020;8(4):e10733.
Berryhill S, et al. Effect of wearables on sleep in healthy individuals: a randomized crossover trial and validation study. J Clin Sleep Med. 2020;16(5):775–783.
Mollicone D, et al. Predicting performance and safety based on driver fatigue. Accid Anal Prev. 2019;126:142–145.
Loncar-Turukalo T, et al. Literature on wearable technology for connected health: scoping review of research trends, advances, and barriers. J Med Internet Res. 2019;21(9):e14017.
Basner M, et al. Fitness for duty: a 3-minute version of the psychomotor vigilance test predicts fatigue-related declines in luggage-screening performance. J Occup Environ Med. 2011;53(10):1146–1154.
Forsman P, et al. Posturographic sleepiness monitoring. J Sleep Res. 2007;16(3):259–261.
Thomas M, et al. Fatigue proofing. In: Kryger MH, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 7th ed. Philadelphia: Elsevier, in press.
Rainey D, et al. Sleep and transportation safety: role of the employer. SleepMed Clin. 2019;14(4):499–508.
Gander PH, et al. 2017. Fatigue risk management systems. In: Kryger MH, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 6th ed. Philadelphia: Elsevier, 2017:697–707.
ACKNOWLEDGMENTS
The shift length task force thanks Dr Claire Caruso (National Institute for Occupational Safety and Health), Dr Michael Hodgson (Occupational Safety and Health Administration), and Emily Whitcomb (National Safety Council) for lending their expertise and providing valuable feedback during the development of this manuscript. While the Occupational Safety and Health Administration (OSHA) does not have concerns with the content of the guiding principles, OSHA does not endorse them. The shift length task force also thanks two anonymous reviewers for valuable feedback on the paper, and Ginger Ellen Espinoza of the Naval Postgraduate School for the graphic design of Figure 1.
Author information
Authors and Affiliations
Corresponding author
Additional information
Address correspondence to: Indira Gurubhagavatula, 3624 Market Street, Suite 201, Philadelphia, PA 19104, USA. Email: indira@pennmedicine.upenn.edu
Appendices
APPENDIX A
Biological Processes of Sleep/Wake Regulation
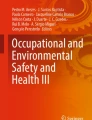
Mental fatigue, as defined earlier in this paper, is influenced strongly by sleepiness, and thereby by time of day and by the durations of wakefulness and prior sleep. This relationship is governed by two primary biological processes: the “circadian” wake drive and the “homeostatic” sleep drive.131–133 During the day, the circadian process produces rising pressure for wakefulness, which counteracts sleepiness. During the night, the circadian process withdraws this wake pressure, which promotes sleepiness and tendency to fall asleep. Simultaneously, during periods of wakefulness, the homeostatic process builds up pressure for sleep, which promotes sleepiness. During sleep periods, homeostatic pressure for sleep dissipates; the longer the sleep period, the less the remaining homeostatic sleep drive. Awakening from sleep occurs naturally when the remaining homeostatic sleep drive is overcome by the circadian wake drive. At any given time during wakefulness, sleepiness—and thereby mental fatigue as defined in this paper—is thus influenced by the interplay between the two processes, as illustrated in Figure A1.

Regulation of sleepiness by two biological processes.
A circadian process (red) produces a rising pressure for wakefulness, which counteracts fatigue, during the day; and a withdrawal of that pressure for wakefulness, thereby promoting sleepiness, during the night. Simultaneously, a homeostatic process (blue) builds up a pressure for sleep, thereby promoting sleepiness, during periods of wakefulness; and dissipated that pressure for sleep (dark gray), thereby providing recovery, during periods of sleep (top panels).131 The combined effect of the circadian and homeostatic processes on sleepiness may be calculated as the net difference between the homeostatic pressure for sleep and the circadian pressure for wakefulness (bottom panels, green),132 as illustrated here for a scenario with a daytime duty period (light blue) and an 8-h nighttime sleep opportunity (left panels) and for a scenario with a nighttime duty period (light blue) with an 8-h daytime sleep opportunity (right panels). Note that in the day work scenario, the sleep opportunity is ended (e.g. through use of an alarm clock) somewhat prematurely, as there is still some homeostatic pressure for sleep left to be dissipated (top left). In the night work scenario, however, sleep is curtailed much more, with the rising circadian wake pressure causing awakening from daytime sleep well before the end of the sleep opportunity. The early awakening leaves a higher level of homeostatic sleep pressure at the end of the shortened sleep period (dark gray) and causes a portion of time available for sleep in this scenario (light gray) to remain unutilized (top right). The combined effect of the two processes—sleepiness calculated as the net difference between the homeostatic pressure for sleep and the circadian pressure for wakefulness—is that sleepiness is low and stable throughout the duty period in the daytime duty scenario (bottom left), whereas sleepiness increases and peaks toward the end of the duty period in the nighttime duty scenario (bottom right). Note that the transient cognitive impairment immediately after awakening known as sleep inertia115 is not depicted in this figure.
Because the circadian process is a function of time of day, while the homeostatic process is a function of time awake and time asleep, the interplay between the two processes depends critically on the timing of periods of wakefulness and sleep. Figure A1 illustrates this for a healthy young adult in a day work scenario with daytime wakefulness and nighttime sleep (left panels), and in a night work scenario with nighttime wakefulness and daytime sleep (right panels). In the day work schedule, the interplay between the circadian and homeostatic processes maintains a stable, low level of sleepiness during most of the day, followed by a rapidly rising level of sleepiness in the late evening leading to the initiation of sleep. Furthermore, during nighttime sleep, the interplay between the two processes produces a consolidated sleep period. If the sleep period is not long enough, dissipation of the homeostatic pressure for sleep may be insufficient, and use of an alarm clock may be needed to wake up in time for work or other responsibilities.
By contrast, in a night work schedule, the interplay between the circadian and homeostatic processes produces a steady increase in sleepiness through most of the night. Furthermore, the rising circadian wake drive during daytime sleep causes early awakening and incomplete dissipation of the homeostatic pressure for sleep. High circadian wake drive during the late afternoon and early evening (the so-called “forbidden zone for sleep”134 or “wake maintenance zone”135) makes it difficult to obtain additional sleep during the afternoon. Thus, compared to a day work scenario, a night work scenario tends to produce sustained sleep loss and dynamically changing, higher levels of sleepiness.13
Given this biological regulation of sleepiness and its impact on mental fatigue, a prescriptive limit on work hours would not, by itself, prevent high fatigue levels during a night work schedule. (In fact, a prescriptive limit on work hours could inadvertently place the commute home at the time of greatest sleepiness, just before the rising circadian wake drive would partially reduce sleepiness again and mitigate fatigue.11)
APPENDIX B
Example Risk and Safety Management Policy Frameworks
Shift duration is a safety and health issue with legal implications, and policies and procedures pertaining to shift duration are best embedded within organizational risk and safety management systems.121 Many industries have pre-existing policy frameworks from which to draw, such as workplace health and safety policies, Safety Management System (SMS) policies, or Fatigue Risk Management (FRM) policies. Here we provide a few links to example frameworks and free resources (shared with permission), which may serve as a starting point for organizations to establish their own policies:
-
The “Fatigue Risk Management Toolkit for Residents, Leaders, and Policy Makers in Canadian Postgraduate Medical Education” document contains practical tools and an implementation guide for managing fatigue in Canadian medical education. In large part it readily applies to U.S. medical education settings. It can be downloaded from: http://www.residentfatigue.ca/mssites/frm/PDF/Fatigue-Risk-Management-Toolkit-WEB5.pdf (last accessed on March 30, 2021).
-
The “FRM Standard Operating Procedure for Utilities” document provides a straightforward but comprehensive standard operating procedure for a fatigue risk management system (FRMS) currently used in Australia. It may be adapted for U.S. operations and can be downloaded from: https://www.sleepresearchsociety.org/wp-content/uploads/2021/03/FRM-Standard-Operating-Procedure-for-Utilities.pdf (last accessed on March 30, 2021).
-
The Fatigue Risk Management Systems Implementation Guide for Operators, 1st edition6 developed by the International Air Transport Association (IATA), the International Civil Aviation Organization (ICAO), and the International Federation of Airline Pilots’ Associations (IFALPA) is widely seen as a model for FRMS in larger operations. It can be downloaded from: https://www.icao.int/safety/fatiguemanagement/FRMS%20Tools/FRMS%20Implementation%20Guide%20for%20Operators%20July%202011.pdf (last accessed on March 30, 2021).
-
The 2018 Fatigue Risk Management Guidelines for Emergency Medical Services Implementation Guidebook helps EMS administrators with the implementation of rigorously developed, evidence-based guidelines52 for fatigue risk management in EMS, with condensed summaries of recommendations and sample policy statements that may be tailored to the needs of local agencies. It can be downloaded from: https://nasemso.org/wp-content/uploads/Fatigue-Guidebook-FINAL-2018Oct.pdf (last accessed on March 30, 2021).
In addition, the “Fatigue at Work Employer Toolkit” developed by the National Safety Council (NSC) contains educational materials for human resources personnel, supervisors, and employees pertaining to fatigue-related safety risks. It can be downloaded from: https://safety.nsc.org/fatigue-risk-management-toolkit (last accessed on March 30, 2021).
APPENDIX C
Recommendations for the Development of Systems to Monitor the Outcomes of Changes in Shift Duration
After making changes in shift duration, organizations should monitor and respond to leading indicators of potential problems and both positive and negative outcomes to ensure the effectiveness of their shift duration policies. Monitoring systems should identify, report, quantify and manage existing and emerging risks. For the development of such systems, the following recommendations deserve consideration:
-
(1)
The degree (and likely cost) of monitoring should be proportional to the anticipated risk level. Where the risk level is low, monitoring may be relatively minimal. Where the risk level is high, however, monitoring should be more comprehensive, evidence-based and, in larger operations, bolstered by third-party oversight.
-
(2)
Monitoring systems should identify and report key performance indicators. These indicators should enable the organization to demonstrate evidence for the following.
-
(a)
There is appropriate knowledge of relevant policies, including personal and organizational roles and responsibilities in identifying, reporting, quantifying and mitigating the risks associated with extended shifts.
-
(b)
There is appropriate training and education of staff in how to identify, report, quantify and manage the risks associated with extended shifts.
-
(c)
Methodologies used for measuring, reporting and mitigating risks are evidence-based, subject to regular evaluation and, where appropriate, modified in light of local experience and/or relevant or emerging scientific evidence. These could include, and are not limited to, measures of
-
∘ planned and actual working time arrangements for all at-risk employees, including planned and unplanned overtime, on-call work, secondary employment, or other activities likely to interfere with sleep
-
∘ sleep-wake behavior of individualemployees, as part of a shared-responsibility framework in which employer and employees have joint responsibility for ensuring adequate sleep
-
∘ fatigue/sleepiness-related changes in behavior or task performance
-
∘ self-report measures of fatigue, sleepiness, alertness, or fitness-for-duty
-
∘ the efficacy and utilization rates of in situ countermeasures at the organizational level.
-
-
(a)
-
(3)
Based on data obtained in (2), organizations should respond appropriately to opportunities to apply corrective actions that will reduce risks associated with shift duration.
-
(4)
Monitoring systems should be cost-effective, so that the costs of implementation, or of the application of corrective actions, does not exceed the likely benefits. This guidance should, however, not be interpreted as advice to minimize resources dedicated to monitoring.
-
(5)
Organizations should implement a system that will enable them to identify and respond to any meaningful relationships between shift duration and risk outcomes including, but not limited to, productivity, performance, safety, health, and community and environmental consequences.
APPENDIX D
Background Information on Countermeasures for Risks Associated with Shift Duration
This Appendix provides background information and references that pertain to selected countermeasures for risks associated with shift duration as shown in Table 1. Implementation of these countermeasures can be complex, and consultation with an expert is generally recommended.
D1. Scheduling Improvements for Shift Work and Extended Shift Operations
Thoughtful and data-driven design of working time arrangements can contribute to risk mitigation by maximizing and protecting sleep opportunities, aligning work schedules with the circadian rhythm of the biological clock, and/or increasing time for recovery after extended duties or multiple shifts. While the primary focus of this paper is on shift duration, the timing of shift starts and ends, and other aspects of the working time arrangements are also important to consider in this regard.136,137 Scientific evidence pertaining to these issues is limited, and conclusive studies of scheduling improvements are largely lacking due to a wide range of possible confounds.138 Nonetheless, the following guidelines provide some insight into what kinds of scheduling practices affect performance, safety, and health risks and therefore present potential opportunities for improvement.
-
Shift systems with backward rotation, in which the start times of consecutive shifts is advancing (i.e. the next block of shift starts at an earlier time of day than the current block), are generally less well tolerated than shift systems with forward rotation or fixed shift times.81 The speed of rotation (i.e. how many shifts in a block with the same start time) also plays a role in rotating shift systems, but the evidence on its effects is mixed.139
-
Both night shifts and early morning starts curtail nighttime sleep opportunities, which increases risk levels relative to late morning and afternoon/evening shifts.77,140
-
Shift durations beyond 12 h in duration tend to be associated with increased risk levels.80,140 Shift durations of 24 h or more without protected opportunities to nap while on duty are not recommended.51 Evidence is mixed, however, on 12-h shifts compared to 8-h shifts.51,141
-
Risk levels tend to accumulate across consecutive shifts without days off.142,143
Double (i.e. back-to-back) shifts and quick returns, overtime, and second jobs increase risk levels.22,144,145
-
Irregular and unpredictable work hours and on-call duty schedules are often perceived as stressors and may also interfere with the ability to obtain adequate sleep, thereby increasing risk levels.9,146
-
Whereas the impact of workload (or task load) is not well established,147,148 high workload may interfere with control over the pacing of work tasks and restrict time for rest breaks, which may increase risk levels.
D2. Napping
Taking a nap—a relatively short sleep period that may be (loosely) defined as less than half the duration of an individual’s typical nocturnal sleep length—is an effective way to supplement the daily amount of sleep and a powerful countermeasure to sleepiness and fatigue.149–153 Naps as short as 15 min and as long as several hours can be effective, whether before work (pre-emptive or prophylactic naps), during work (on-the-job or strategic naps), or after work (catch-up naps).112,154–156 Naps may facilitate adaptation to a shift work schedule and ease the return to daytime activity,157,158 and may offer cardiovascular health benefits.159,160 Split sleep schedules, in which a person takes a nap after a work shift and another nap before the next shift, have been associated with increased sleepiness,161 but few differences in performance relative to a consolidated post-shift sleep bout.162,163 For on-the-job napping to be implemented successfully as a countermeasure strategy, it is important that it be sanctioned164 and that there is access to a safe and quiet place to rest while on break.109,127
Importantly, napping may produce post-nap sleep inertia, a transient feeling of grogginess and impaired performance immediately upon awakening.115,165 Sleep inertia can be particularly problematic in on-call settings146 and may require a worker to delay the return to work for up to about 30 min after waking.166,167 Sleep inertia may be less intense after shorter (approximately 10–30 min) naps, but scientific evidence on this matter is inconclusive.168 Caffeine consumed just prior to a nap appears to be an effective countermeasure to performance impairment due to sleep inertia immediately after the nap.129 (see Appendix D3).
D3. Caffeine Use
There is abundant evidence that caffeine reduces sleepiness and fatigue and mitigates deficits in cognitive performance.116,169 When caffeine is used in conjunction with a nap, it may also reduce the time to overcome post-nap sleep inertia.170–173 Caffeine is widely available and found in many drinks and foods, either naturally occurring or as an additive; furthermore, caffeine can be obtained in the form of chewing gum and various over-the-counter medications. Available evidence suggests that moderate use of caffeine is compatible with a healthy lifestyle.174
The pharmacodynamics of caffeine are poorly understood, and large inter-individual differences in caffeine sensitivity, effectiveness, habituation, and tolerance exist.175–177 This limits the ability to provide tailored advice regarding dosing of caffeine to mitigate fatigue - although given the widespread presence of caffeine in foods and drinks, precise dosing could be difficult in practice regardless. Even so, the preponderance of scientific evidence indicates that caffeine is an effective fatigue countermeasure, and access to caffeine as part of a comprehensive fatigue risk management program is recommended.111
Caffeine present in the bloodstream just before bedtime may delay sleep onset and reduce the quality and quantity of subsequent sleep, although individuals differ considerably in their sensitivity to these effects.178 Sustained use of high-dose caffeine can cause additional undesirable effects, including anxiety, tremor, arrhythmias, insomnia, dehydration, and withdrawal headaches.179,180 For healthy adults, caffeine consumption up to about 400 mg per day (300 mg per day in pregnant women) is generally considered safe;181 however, the decision to use caffeine and the amount and frequency of use should be based on individual assessment of benefits versus undesirable side effects.
D4. Sleep Hygiene and Treatment of Sleep Disorders
Sleep disturbances that are not necessarily related to the work environment contribute to work-related errors and injuries.182 Sleep hygiene, which refers to a set of behavioral and environmental recommendations intended to promote good sleep,183 can help to obtain adequate duration of quality sleep. The recommended amount of sleep for the average adult is 7 h per night or more.105,106 Achieving this on a regular basis provides some degree of resilience against the adverse cognitive effects of subsequent sleep loss.184,185
Sleep hygiene environmental recommendations, which pertain to personal sleep spaces as well as any workplace sleep facilities, include ensuring a comfortable, appropriately sized bed; minimal light exposure and noise; comfortable temperature and humidity; and no sleep interruptions (unless there is an emergency).186,187 Sleep hygiene behavioral recommendations found in the literature, which are primarily focused on the habitual sleeping environment, include maintaining regular bed and wake times; avoiding daytime naps; avoiding bright light exposure during the 2–3 h prior to sleep; avoiding large meals or alcohol consumption for at least 2 h prior to bedtime; avoiding strenuous exercise immediately before bedtime; and avoiding caffeine, nicotine, and other stimulants for at least 6 h before bedtime.187,188
In operational settings, some or all of the behavioral recommendations may not be feasible or practical to implement (e.g. because irregular work schedules may interfere with maintaining regular bed and wake time) and may actually be at odds with effective fatigue risk management (e.g. because taking a daytime nap may be needed to mitigate fatigue). That is, some of the behavioral recommendations could be counterproductive for getting enough sleep or ensuring optimal performance and safety (especially in shift work settings). Also, although they are worthy sleep health recommendations in their own right, evidence of their effectiveness with regard to workplace performance, safety and health is limited.188 The behavioral recommendations should therefore not be seen as advice against pursuing catch-up sleep or naps, or using bright light or caffeine prior to bedtime, when doing so would be the better choice for safety.
Sleep disorders (e.g. obstructive sleep apnea, insomnia), medical conditions (e.g. diabetes mellitus, gastroesophageal reflux disease, back pain), and psychiatric disorders (e.g. depression, post-traumatic stress disorder) can transiently or chronically reduce the quality and quantity of sleep.189 For affected workers this can result in poor sleep quality, insufficient sleep, or excessive sleepiness, which can then negatively affect work performance. Additionally, some medications (e.g. hypnotics, antidepressants) incur side-effects that contribute to increased risk of fatigue during work hours, either through direct effects on sleepiness, or indirectly by worsening sleep quality or decreasing sleep duration.190 Workplace education regarding sleep disorders, treatment, and implications for safety and well-being has been found to reduce risk of occupational injuries.191 Furthermore, an employer-supported sleep disorder (obstructive sleep apnea) treatment program in the U.S. trucking industry has been shown to yield significant benefits in terms of crash risk, driver retention, and medical insurance costs.192,193
D5. Wake- and Sleep-Promoting Medications
Wake-promoting (stimulant) and sleep-promoting (hypnotic) medications should be used in consultation with and under supervision of a medical provider with expertise in management of sleep/wake disturbance associated with non-traditional work hours. A discussion of their pharmacological and clinical specifications is beyond the scope of this paper but can be found in the literature.194,195 The advantages and disadvantages of wake- and sleep-promoting medications and the legal and ethical considerations for their use in operational settings have also been discussed in the literature.123,196 Certain occupations have regulations or policies that prohibit the use of some or all of these medications.
Use of wake-promoting medications may interfere with the ability to obtain adequate sleep after bedtime.197 Use of sleep- promoting medications may result in next-day residual sedation, which could impair performance while at work or commuting to work,198 although caffeine intake may be helpful to mitigate this effect.199 Long-term use of wake- or sleep-promoting medications may have unintended effects on sleep, mood, and health.195,200 Interactions with other medications or with alcohol201 may increase the risk of side effects from wake- or sleep promoting medications. Alcohol, which some individuals use as a sleep aid, may degrade sleep quality, exacerbate sleep apnea, and cause next-day sleepiness.202
Melatonin, which in the United States is available over the counter as a dietary supplement, is usually marketed and used as a sleep aid. However, the primary effect of melatonin—a hormone that is also naturally produced by the pineal gland during the evening and night—is that it can shift the timing of the biological clock.203 As such, melatonin may be used to help realign sleep-wake timing and facilitate daytime sleep for night shift workers204 or to help overcome jet lag after travel across time zones.205 Optimizing the timing of melatonin administration is critical to achieving the desired effect, with morning administration leading to delays of the biological clock (shifting sleep later) and evening administration leading to advances of the biological clock (shifting sleep earlier).206 This makes achieving optimal effectiveness complicated in practice, and mistimed melatonin administration may even result in the opposite effect of what is desired. Melatonin use is generally considered safe and side effects are minimal,207 but it is not regulated in the United States and may contain additives with adverse health effects. As with other sleep-promoting medications, a medical provider with expertise in management of sleep/wake disturbance associated with non-traditional work hours should be consulted if melatonin is considered as a potential aid for sleep difficulties in the context of working time arrangements.
D6. Bright or Blue Light Exposure
Light has the potential to shift the biological clock, and it also affects alertness.208 Morning light exposure causes the biological clock to advance (shift earlier), and evening light exposure causes the clock to delay (shift later).209,210 The magnitude of these effects depends on the duration, brightness, and color of light exposure. The brighter the light and the longer the exposure, the greater the shifting,211,212 and light that is blue or blue-enriched is particularly effective for shifting the biological clock.213 Based on these principles, manipulation of light exposure can be used to shift the biological clock by some desired amount of time, for example to facilitate adaptation to a shift work schedule.214 Optimizing the timing of light exposure is critical to achieving the desired effect.208
The biological clock tends to shift no more than a few hours per day. This approach to shift work adaptation would therefore only work well for fixed or slowly rotating shift schedules, in which shift start or end times are expected to occur at approximately the same time for several consecutive days. Even then, additional measures may be required, such as wearing dark goggles or using technological solutions to reduce bright or blue light exposure at certain times,215 making the desired effect difficult to achieve.216 Strategies for mitigating risks in shift workers that rely on minimization of extended wakefulness and sleep loss, rather than shifting the biological clock, may be more effective in practice.
Light exposure has an acute alerting effect.217 To some extent the magnitude of this effect depends on the brightness level of the light,218 and light that is blue or blue-enriched is particularly effective for promoting alertness.219 Little is known about how long the alerting effect of light exposure lasts after the exposure has ended.220 That said, use of blue- enriched white light in the workplace has been reported to improve alertness, performance, and sleep quality.221 The acute alerting effect of light, however, cannot be separated from its effects on the biological clock. Especially in shift work settings, therefore, individuals exposed to bright or blue light to improve alertness may also experience a shift of the biological clock, which may or may not be problematic depending on the situation. Furthermore, inappropriate light exposure has the potential to adversely affect sleep. In many situations, therefore, light may not be a suitable countermeasure for risks associated with shift duration.
Exposure to light at night associated with shift work has been found to increase the risk of cancer.222–224 Additionally, chronic exposure to bright or blue light therapy has been linked to retinal damage later in life.225,226 This finding awaits corroboration with additional clinical studies.
D7. Exercise and Activity Breaks
In addition to the well-known benefits of physical activity from exercise and activity breaks with regard to skeletomuscular and overall health and wellness, physical activity has some potential to improve sleep.227,228 However, exercise less than 1 h before bedtime may delay sleep onset.229 Exercise also has the potential to shift the biological clock, with morning exercise facilitating advances and evening exercise facilitating delays of the biological clock.230 In the laboratory, nightly bouts of exercise have been found to promote adjustment of the biological clock to a night shift schedule.231
During sleep deprivation, physical activity may produce a modest short-term reduction in subjective sleepiness, but there may not be any concomitant improvement in cognitive performance.232 A review of continuous exercise at active workstations found minimal evidence for increased workplace performance or productivity.233 The extent to which exercise can be used effectively as a fatigue or risk countermeasure in operational settings remains to be investigated.
D8. Fatigue Prediction, Detection and Warning Technologies
Technologies available to help manage risks from fatigue can be broadly categorized as biomathematical models of fatigue,234 tools for monitoring sleep and sleep debt,235 tools for detecting and warning about fatigue,236 and fitness-for-duty tests.237 Biomathematical models of fatigue make use of equations describing the regulation of sleep and wakefulness and the biological clock to provide predictions of sleepiness or performance impairment for a (hypothetical) average individual, based on a given sleep schedule or work schedule.238,239 Use of these models is commonplace before, during and after duty periods in commercial and military aviation,240,241 where shift scheduling is typically tightly managed. However, they are deemed to be of more limited utility in settings where shift scheduling is on demand or otherwise less strictly under operational control.242
Tools for monitoring sleep have become widely available in the consumer market over the last decade. Frequently integrated with physical activity and health monitoring systems, they usually consist of wearable sensors coupled with a smartphone-based software application.243 Such tools do not usually meet professionally accepted criteria for sleep assessment,244 but have been found helpful in allowing individuals to monitor and potentially improve their sleep245 or potentially seek medical evaluation. Tools for monitoring sleep may also serve to determine a person’s sleep schedule for use with a biomathematical model of fatigue in order to predict impending safety risks.246 A significant challenge with wearable technologies is user acceptability; people often do not tolerate wearing additional devices, especially if they are uncomfortable or obtrusive, interfere with work, or do not also fulfill other useful functions.247
Tools for detecting and warning about fatigue, commonly referred to as fatigue (or drowsiness) detection and warning systems, are manifold and diverse. Technologies for fatigue detection aim generally to measure fatigue continuously from unobtrusively observable signals that correlate with fatigue, such as various ocular measures, sleepiness-related variables derived from the electroencephalogram (EEG), indices of heart rate variability, changes in speech and voice, or facial expressions. A diversity of modalities for providing fatigue warnings have been implemented, including visual, auditory, and haptic alerts as well as warning messages transmitted to third parties for possible intervention. In cars and trucks, fatigue and error detection systems may activate driver assist technologies to help avoid accidents.69
In contrast to fatigue detection and warning systems, tests for fitness-for-duty (or readiness-to-perform) typically provide snapshot measures of fatigue and often require an individual’s active involvement such as performing a reaction time task248 or taking a balance test.249 While fatigue testing for fitness- for-duty provides an instant, objective estimate of a person’s level of fatigue, such testing does not track subsequent changes in fatigue over time unless the test is conducted repeatedly (although such changes could conceivably be predicted using a biomathematical model). Most fitness-for-duty tests are not specific for fatigue; other sources of impairment (e.g. distraction, alcohol intoxication) produce similar test results. For fitness-for- duty tests that rely on user response to assess fatigue, variations in motivation and effort may also influence test results.
Fatigue prediction, detection and warning technologies that have been shown to be both sensitive and specific to relevant levels of fatigue are rare. However, both of these accuracy attributes are important. Technologies need to be sensitive enough to detect or predict levels of fatigue that compromise performance and safety, as failures to identify these could have critical, even fatal consequences. At the same time, technologies need to be specific enough not to inadvertently trigger alerts when fatigue levels are low, as too many false alarms will quickly desensitize the user. Many of the currently available technologies are proprietary, and the extent to which they have been subjected to independent research is often limited. For most of these technologies, publicly accessible data on accuracy, reliability, and validity are limited or unavailable.
Collection of objective data in operational settings may have important implications for privacy and could carry liability for employers and employees. For example, following an accident in which fatigue is suspected to be a main contributor, sleep monitoring data may be subpoenaed to determine the amount of sleep obtained prior to the accident. This potential issue notwithstanding, when used as part of a comprehensive fatigue risk management system, fatigue prediction, detection and warning technologies may contribute to a worthwhile, data- driven process of continuous improvements in risk mitigation (see Appendix D9).
D9. Risk Mitigation Tools, Policies, and Practices
Even though shift duration and its attendant fatigue may be the source of risks to performance, safety, and health, countermeasures do not necessarily have to address the source of these risks to mitigate the risks themselves.70 There are many possibilities for “fatigue proofing” that mitigate or avoid risks through other means,250 such as use of task checklists and standard operating procedures (e.g. for end-of-shift hand-offs),5 team work strategies,29 extra staffing,144 scheduled rest breaks,81 providing safe transportation options after work shifts,251 engineering solutions (e.g. safety valves in factories, rumble strips on the road, automation in the operation of machines),5 and implementation of safety policies, procedures, and management systems23 (see also Appendix B). Furthermore, an educated workforce is a key component of risk mitigation. Fatigue risk management training should help workers, their managers, and other operational personnel (e.g. scheduling, human resources) understand how to manage work, sleep, and the application of countermeasures in order to maximize performance, safety, and health.122
Fatigue risk management training and other risk mitigation strategies may be incorporated into a fatigue risk management system (FRMS), which is a proactive, data-driven process whereby an organization undertakes a formal risk management approach to reducing the effects of fatigue in the workplace.121,252 An FRMS program involves all stakeholders (workers, management, unions, regulators), includes proactive data collection steps, and adapts to dynamically changing risks so as to be self-improving. The implementation of a FRMS is unique to the needs of a given industry and company, but the elements of FRMS programs are similar across industries (see also Appendix B). A FRMS is often embedded within a larger safety management system (SMS) to allow for integrated risk management. FRMS program managers are typically responsible for developing and implementing policies designed to mitigate fatigue-related risks (e.g. scheduling and rest requirements, and countermeasure use), investigating fatigue-related incidents and accidents, monitoring safety performance indicators, evaluating the impact of work schedules on performance and safety, providing mechanisms for individuals to report fatigue at work, providing recommendations for modifying schedules to improve fatigue-related outcomes, and providing regular training and resources to employees on best practices for managing work, sleep, and the application of countermeasures.121,124
Rights and permissions
About this article
Cite this article
Gurubhagavatula, I., Barger, L., Barnes, C. et al. Guiding principles for determining work shift duration and addressing the effects of work shift duration on performance, safety, and health: guidance from the American Academy of Sleep Medicine and the Sleep Research Society. J Clin Sleep Med 17, 2283–2306 (2021). https://doi.org/10.5664/jcsm.9512
Received:
Accepted:
Published:
Version of record:
Issue date:
DOI: https://doi.org/10.5664/jcsm.9512
